

Prenatal Genetic Testing
A Death Cult Trap to Increase Abortions for Tissue Harvesting

The current modern cultural system is diseased. It profits from death, manipulation, corruption, and lies. Fear and ignorance are used to manipulate outcomes in favour of big industry that uses baby body parts to manufacture fraudulent products such as vaccines or other unnecessary drugs. I will lay out my discussion here on how prenatal genetic testing is one such funnel leading to desired industry outcomes, and how to steer clear of this machine, with all its arms of attack on what is good, true, pure, and holy, carried out in the name of power, control, manipulation, and false ideology.
Prenatal genetic testing, particularly non-invasive prenatal testing (NIPT), is widely promoted as an accurate way to detect chromosomal abnormalities. In reality, these tests are not diagnostic and carry significant false positive rates. The diagnostic aspect is meant to come after a positive NIPT, but that, too, is wrought with problems. The FDA has issued safety communications warning that many NIPTs are marketed without regulatory review and that positive results must be confirmed with diagnostic procedures such as amniocentesis or chorionic villus sampling. Studies show that false positives are far more common than false negatives, especially for rare conditions such as Trisomy 13, Trisomy 18, and sex chromosome abnormalities, with positive predictive values often below 50 percent in low-risk populations.
Examples of misdiagnosis are well documented. Many women have been told their babies had Trisomy 18 and were urged to terminate, only to later deliver healthy children. Motherly reported a case where a woman was told her baby had Trisomy 18, but the diagnosis was incorrect, and the child was healthy. As I have taught for many years, screening tests and doctors’ opinions of such are dangerous. They can cause unnecessary fear and stress in the parents and can lead the family down a false path of ever-increasing tests and meddling, leading to poor birth outcomes. All it takes is a suggestion that there is a problem, and then come the waves of opinions and “just in case” testing that can lead parents into more unnecessary interventions. A family that wants a natural homebirth could easily be fear mongered into a hospital birth or C-section.
The organisation Compatible With Love has collected multiple stories from mothers who were given positive results for Trisomy 18 but delivered unaffected babies. Parents magazine reported on an analysis done by The New York Times showing that 85% of NIPTs were inaccurate. Another case involved a suspected Turner syndrome diagnosis, later proven false, with the child born without abnormalities. FaithPot documented a family who were told their baby had spina bifida, yet the child was delivered healthy.
The FDA says they are aware of cases where people have terminated pregnancies for medical reasons based on results of NIPT false positives, where the fetuses are later found to be healthy.
Genetic non-invasive prenatal screening tests may have false results: FDA safety communication. U.S. Food and Drug Administration. 2022.
When I was pregnant at age 36, my partner wanted to know the sex of our baby, so I agreed to have one ultrasound. That one turned into two because they found I had a single umbilical artery (SUA) instead of the more usual double, and automatically suggested I could have a child with Down syndrome or other issues. The midwives demanded I go to a cardiologist for another scan to rule out a heart condition. I went to the appointment, and of course, nothing was wrong, but I had a fascinating conversation with the irritated doctor who told me it was ridiculous that I was sent for this scan because: a SUA was a normal variation that did not mean Trisomy, in fact all the one’s he had seen had two arteries, and that most Down children come from teen pregnancies rather than “geriatric” ones.
False positives occur for several reasons, including confined placental mosaicism, vanishing twin DNA, maternal chromosomal variations, and laboratory error. Because these tests analyse placental DNA fragments circulating in maternal blood, they do not directly assess the genetics of the fetus. As a result, abnormal results may reflect the placenta or maternal tissue rather than the child.
Despite these limitations, many practitioners present NIPT results as definitive. The effect is the manipulation of pregnant women through fear, leading some to end pregnancies based on inaccurate information. This constitutes a misuse of science and highlights the ethical dangers of deploying imperfect screening technologies as tools of persuasion rather than as optional information sources requiring cautious interpretation.
The Diagnostic Step (or Misstep?)
Amniocentesis and chorionic villus sampling are invasive procedures used to confirm results from prenatal screening tests, and both carry well-documented risks that are often minimised during counselling. Amniocentesis involves inserting a needle through the abdominal wall into the uterus to extract amniotic fluid, while CVS removes placental tissue either through the cervix or the abdomen. These procedures carry a measurable risk of miscarriage, which large reviews estimate at roughly 1 in 300 to 1 in 500 for amniocentesis, with CVS generally showing a slightly higher risk, particularly when performed earlier in pregnancy. Additional risks include “infection” (aka contamination), bleeding, rupture of membranes, Rh sensitisation, and injury to the fetus. CVS has also been associated with limb defects when performed very early, and both procedures can trigger inflammatory responses that compromise pregnancy stability.
Beyond physical risk, there are systemic and ethical concerns. These confirmatory tests are frequently positioned as neutral diagnostic tools, yet they function within a decision-making pathway that often presumes termination as the logical next step if an abnormality is detected. In many cases, the conditions being tested for are not treatable in utero, meaning the information gained does not improve outcomes for the child but instead increases psychological pressure on parents during a vulnerable period. False positives and ambiguous findings can further escalate fear, leading to invasive testing that may never have been necessary. In this way, amniocentesis and CVS often serve less as protective medical tools and more as reinforcement mechanisms within a broader prenatal screening system that channels pregnancies toward predetermined institutional outcomes rather than informed, supported choice. Just like you would expect from the death cult.
PCR Problems
Prenatal genetic testing relies heavily on PCR, which, especially since fake COVID, has been falsely elevated into the realm of diagnostic authority when it was never designed for such a role. The polymerase chain reaction is essentially a simple DNA photocopier, one I used often when I was working on my science degree at the University of Lethbridge. It amplifies fragments of nucleic acids through cycles of heating and chemical reactions, generating synthetic copies in bulk. The method is extremely sensitive, which means it can detect the tiniest trace of material, but this is also its downfall. There is no standardisation across laboratories for cycle thresholds, specimen collection devices, extraction methods, or even which fragments of DNA are targeted. Cycle thresholds differ widely, and the higher the number of cycles, the more meaningless the signal becomes. Different labs, using different reagents, extraction kits, and targets, can produce entirely different results on the same sample.
The reliance on PCR as evidence of disease ignores these inherent limitations. A signal generated after 35 or 40 cycles of amplification does not mean that the original specimen contained a functional genome or anything capable of causing illness. It simply means that fragments of genetic material were copied enough times to be detected by a machine. Calling this evidence of a medical condition is scientifically unjustifiable. The variability in methods ensures irreproducibility, and the lack of universally applicable cycle threshold values leaves the entire practice vulnerable to manipulation. Genetic theory itself assumes that these snippets of DNA or RNA, often incomplete and contextless, equate to agents of disease, yet there is no proof of causality. What we are left with is the misuse of a chemical copy machine presented as hard evidence used to fear-monger, and an entire industry built on unvalidated assumptions.
Genetic theory takes this one step further by assuming these fragments equate to pathological certainty, even when there is no reproducible causal proof. In the case of prenatal screening, these assumptions are magnified into fear-inducing diagnoses that often collapse under closer examination. Women are not told that the foundation of this testing rests on a chemical photocopier prone to variability and error. They are told it is the truth, something to be worried about, even when it is only the replication of fragments and the interpretation of patterns that may or may not reflect reality in the child.
PCR Contamination Issues
Contamination is a fundamental problem in genetic testing workflows. Laboratories handling cell-free DNA or fetal material are working with extremely low template concentrations, which makes them highly vulnerable to trace contaminants. Environmental DNA, aerosolised amplicons from previous PCR runs, and cross-sample carryover can all introduce extraneous sequences into reactions. Once contaminants are present, amplification cycles replicate them alongside authentic fragments, embedding false material directly into the data.
Cell culture history demonstrates how pervasive this issue can be. Misidentified or cross-contaminated cell lines have been reported for decades. A classic example is the discovery in 1967 that many supposed human and animal cell lines were in fact HeLa cells. Despite this, contaminated lines continued to be used and published into the early 2000s, generating thousands of papers built on incorrect assumptions. This illustrates the persistence of contamination in research environments even under professional standards.
In molecular assays, contamination arises from multiple points. Specimen collection devices can leach DNA from previous manufacturing runs or from operator handling. Pipettes, benches, and gloves accumulate microscopic residues that can transfer between samples. Reagent lots can contain low-level nucleic acid contamination introduced during synthesis. Once any of these are introduced into a low-copy sample, PCR will faithfully multiply them into dominance. This produces false signals that can be indistinguishable from an authentic template without extensive controls.
In prenatal genetic testing, contamination has several specific consequences. Maternal DNA already overwhelms fetal fragments in plasma, so even minor environmental DNA can further distort the fetal fraction estimate. Cross-sample contamination can make one patient’s chromosomal pattern appear in another, leading to erroneous copy number calls. Amplicon carryover from previous runs can mimic rare variant signals, which algorithms may classify as fetal abnormalities. Because the interpretation depends on small shifts in representation, contamination at the level of a few molecules can be enough to trigger a positive screen.
Standard precautions include unidirectional workflow, physical separation of pre- and post-PCR areas, the use of uracil-N-glycosylase systems to degrade carryover amplicons, and environmental monitoring with no-template controls. Even with these safeguards, reports continue to document contamination events that affect clinical calls. Each reagent change, laboratory move, or equipment replacement requires re-validation to ensure contamination has not been introduced into the workflow. The sheer sensitivity of PCR makes absolute prevention impossible, which means contamination remains an intrinsic risk in every amplification-based test.
Stem Cell Regeneration
A note on “stem cells”. My current theory is that what modern science calls stem cells are actually born of the 16-stage pleomorphic somatid cycle described by Gaston Naessens.
Here is the general idea in the table below. I will save the deep dive for another article.
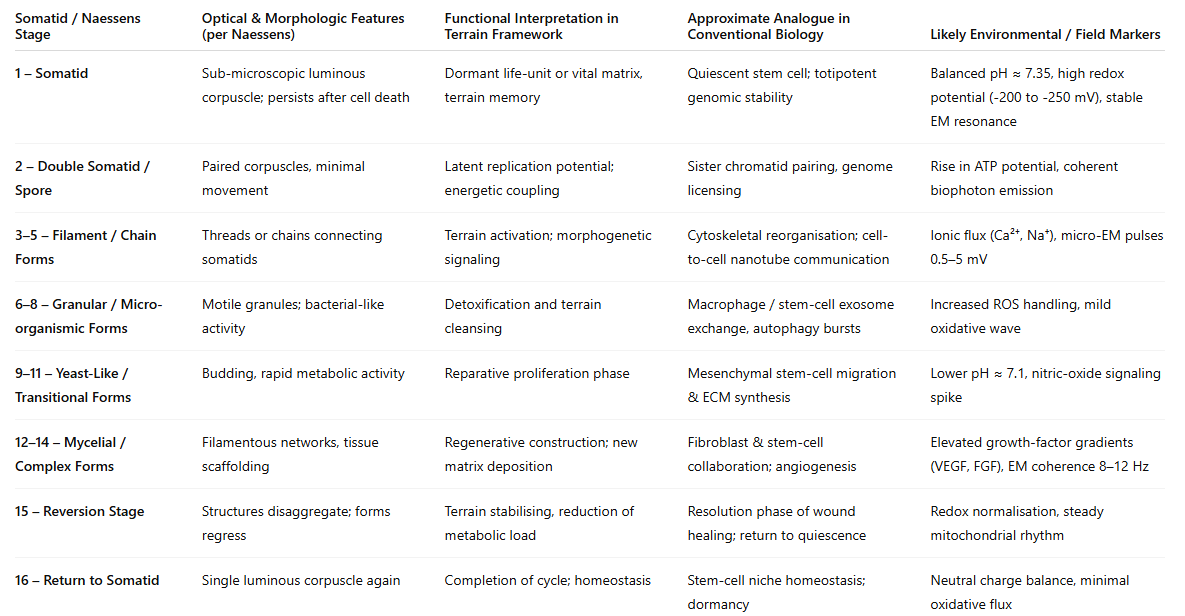
Fetuses and newborns possess extraordinary regenerative capacity because of their stem cell populations. Hematopoietic stem cells and mesenchymal stem cells circulate at far higher levels in fetal and neonatal blood than in adults. Cord blood contains abundant pluripotent precursors that are capable of differentiating into multiple tissue types. This is why cord blood banking exists as a medical industry: the newborn period is a unique window where stem cells are at their peak availability and potency.
During fetal development, injuries and structural abnormalities often correct themselves because of this stem cell–driven plasticity. Studies of congenital anomalies demonstrate spontaneous resolution in utero, including cardiac septal defects, urinary tract obstructions, and pulmonary lesions. The mechanism is high cellular turnover and continuous remodeling, supported by stem cell integration into damaged tissues. Amniotic fluid itself contains stem cells with broad differentiation potential, and these cells migrate to sites of injury within the fetus.
Newborns continue to display repair processes that adults cannot replicate. Neonatal liver and skin regenerate more rapidly, fractures heal at accelerated rates, and central nervous system injuries demonstrate plasticity linked to higher concentrations of progenitor cells. Cord blood stem cells have been investigated clinically for the repair of ischemic brain injury, type 1 diabetes, and cerebral palsy, showing measurable benefits in early trials.
This regenerative system also explains why predictions of deformity or disease from prenatal testing can be overturned by the time of delivery. A genetic screening result reflects fragments amplified in a laboratory; it does not account for the living organism’s ongoing repair processes. Fetuses with flagged abnormalities have been documented to self-correct through stem cell–mediated remodeling before birth. What appears as a permanent defect in amplified DNA data can be transient in reality.
Stem cells are therefore central to understanding why prenatal predictions often fail. The developing child is not a static genome but a dynamic system actively repairing, correcting, and remodeling tissues. Ignoring this reality leads to deterministic claims that a baby will be malformed or diseased, when in fact the biology of development contains inherent healing power that no test can measure.
Medical Cult Fear Programming
Fear is built into the structure of prenatal genetic testing. Women are told from the start that their pregnancies must be monitored and measured against statistical norms. When a test returns a positive flag, it is rarely presented as a possibility with wide margins of error but as an impending certainty. The emotional weight of phrases like “incompatible with life” or “severe abnormality” can override rational discussion. Mothers are placed in a vulnerable state where the fear of carrying a damaged child is amplified beyond the evidence.
This fear is a mechanism of an even deeper rot. False positives are well documented in non-invasive prenatal testing, yet the communication around results continues to emphasise worst-case outcomes. The language is deterministic, the counselling tilted toward termination, and the family is left in a position where choosing life requires defiance of medical authority. It is the same strategy seen in other branches of medicine where uncertain data are leveraged to secure compliance: create the sense of danger, then present intervention as the only safe option.
By manipulating women at their most vulnerable, prenatal testing functions less as a tool of empowerment and more as a psychological lever. Decisions made under pressure and fear often cannot be reversed. This is the human cost of treating unreliable screening assays as definitive truth, and it exposes the core of the system: the underlying death cult programming.
The Death Cult Machine
The death cult framework becomes visible when you trace who built the modern system of prenatal screening and genetic determinism. Science was supposed to be neutral and exploratory, but we are well aware that bias, agenda, and business are at the epicenter. The institutions that shaped this industry were financed and guided by the same Rockefeller foundations that engineered the pharmaceutical paradigm in the twentieth century. Their model is reductionist by design, turning life into fragments and sequences, removing context, and replacing holistic understanding with laboratory control. Genetic theory is a cornerstone of this architecture: the claim that destiny is written in code, that fragments of DNA are immutable and define fate, and that intervention by specialist experts is a requirement to manage that destiny.
When non-invasive prenatal testing is promoted as an absolute or weighted certainty, it feeds directly into the logic of termination. The death cult has been feeding the idea of death as compassion for a long time. False positives, known and acknowledged, become acceptable collateral in a system where the aim is mind and population control. Malthus and Sanger come to mind.
Each flagged abnormality increases the possibility of the death cults’ wet dream: abortions, which is then justified as medical prudence. Behind this front are the industries that profit from fetal tissue, organ trafficking, and research supply chains built on aborted material. This is not a speculative argument. Fetal cell lines such as HEK-293 and WI-38, harvested from elective abortions, are embedded in vaccine development, drug testing, and laboratory research worldwide. These industries require a continuous source of tissue to maintain operations.
The cultural programming is backed by demented ideas. Women are conditioned to believe their babies are risks until proven otherwise, and laboratories are granted authority to dictate the terms of life. Fear is weaponised toward compliance, and compliance feeds the supply lines of a system that consumes life under the banner of science.
The abortion industry has been framed publicly as a matter of women’s rights, while simultaneously supplying a largely hidden downstream market that relies on aborted fetal tissue for research, testing, and pharmaceutical development. Prenatal genetic screening functions as one of several entry points into this pipeline. The Rockefeller death cult built the framework and continues to profit from the demise of innocents.
Xenotransplantation
I will now be sharing a series of videos presenting evidence related to organ harvesting. A content warning is advised, as the material may be distressing.
Here is Dr. Stanley Plotkin, known as the “Godfather of vaccines,” in a deposition
on January 11, 2018, admitting the use of tissue from 76 aborted fetuses for ONE study, all of which were three months or older and normally developed. Many of you may already be familiar with this interview.
He also admitted to using orphans to study experimental vaccines, as well as mentally handicapped individuals and the babies of mothers in prison. He is a self-proclaimed atheist.
Clementine’s Voice is a public testimony by the father of an aborted child, Clementine, detailing what he later discovered was done to his daughter’s body following the procedure. Through records, documentation, and his own investigation, he describes how her organs and tissues were dismembered, catalogued, and distributed for research and commercial use without his informed consent. His account exposes the disconnect between the language used around abortion and the reality of what occurs afterward, highlighting how fetal remains can become commodities within biomedical and pharmaceutical systems.
Multiple investigations and whistleblower accounts have raised serious concerns about practices within Planned Parenthood related to the procurement of fetal tissue. Recorded conversations, internal documents, and congressional inquiries have alleged that, in some cases, fetal demise procedures were altered or delayed in order to obtain intact organs and tissue for research and commercial use. These reports describe situations where standard protocols intended to ensure fetal death prior to tissue retrieval were not consistently followed, raising profound ethical and legal questions.
In 2015, undercover video footage released by the Center for Medical Progress captured senior Planned Parenthood officials discussing methods to obtain specific organs, pricing structures for fetal tissue, and procedural adjustments that could increase tissue viability. Subsequent investigations, including a U.S. Senate Judiciary Committee referral, cited evidence suggesting that fetal tissue procurement was treated as a logistical and financial consideration rather than an ethical boundary. While Planned Parenthood has publicly denied wrongdoing, the documentation reveals a stark contrast between public messaging and internal discussions.
What Can We Do About This?
Step one: understand their agenda and walk away from their cult. Take sovereignty over birth itself. Free birthing, guided by trust in physiology, ancestral knowledge, and the terrain-based perspective, removes the control of OBGYNs and their machinery. Pregnancy is not a pathology! It is not an emergency, it is an emergence. It does not require surveillance by those trained by the death cult in white coats.
Birth requires peace, calm energy, and inward connection. You are never to engage a woman’s neocortex during childbirth! We give birth from our limbic system. This means that if birth is interrupted by asking questions, poking and prodding, having logical conversations, filling out forms, or the like, you are taking a woman out of her limbic system and risking the birthing process.
Learn about birth! I recommend the FreeBirth Society and Eyla Cuenca over at Uncovering Birth. I have plenty of videos on the topic on my website Yummy.Doctor.
The second is to refuse genetic testing altogether. The tests do not offer any helpful guidance; they offer fear and doubt. Opting out denies the system its foothold. A mother who does not submit her blood or her body to their protocols cannot be trapped in their statistics or pressured into their procedures.
Learn about your body so you can avoid an unwanted pregnancy. Check in with your body in case you miss a period to catch an early pregnancy. You can naturally flush away the uterine lining extremely early and safely with high doses of vitamin C and black cohosh. I make a Neem Lubricant that can help prevent pregnancy without poisoning yourself with birth control pills. Vow to never have an abortion. Take responsibility for your fertility without becoming a murderer. There are massive spiritual consequences for these actions. Stop feeding the death cult machine.
Clean eating is the foundation. A body free of toxic residues and nourished with whole, natural foods creates an environment where conception and pregnancy are successful without risk of anomalies. Cleansing before conception is critical. Removing stored chemical loads, supporting liver and kidney drainage, restoring mineral balance, and addressing stagnation to ensure that the terrain is ready to sustain new life. I offer detox courses at Yummy.Doctor.
Stress management is non-negotiable, I know, a tall order these days. Chronic stress alters hormonal communication, nutrient absorption, liver function, and toxin release. Practices of grounding, daily movement, breathing, and alignment with natural cycles protect both mother and child.
Real autonomy means free birthing or homebirthing with a midwife and without OBGYNs whatsoever, with no genetic testing, no ultrasounds, and zero interventions, as one always leads to another. These healthy practices dismantle the fear architecture and restore pregnancy to what it truly is: a natural process requiring trust, inner connection, and wise decisions. We must stop handing our infants over to the murder machine. Let the system starve.
About Dr. Amandha Dawn Vollmer (ADV)
Dr. Amandha Dawn Vollmer (ADV) is a leading voice in terrain-based medicine and one of the foremost authorities on the therapeutic applications of Dimethyl Sulfoxide (DMSO). With a Bachelor of Science in Agricultural Biotechnology and a Doctorate in Naturopathic Medicine (2008), she has dedicated nearly two decades to researching, practicing, and formulating natural remedies that align with the body’s innate design for repair and renewal. She took the value from her academic training, then unschooled herself and walked away from the institutions to pursue truth outside their limitations.
She is the best-selling author of Healing with DMSO, a practical and accessible guide that provides clear instructions, recipes, and protocols for the safe and effective use of this extraordinary substance. As a master formulator, Amandha creates unique, handcrafted remedies and DMSO-based blends that support tissue healing, oxygenation, pain relief, and detoxification. Her work is rooted in a clear understanding of terrain health, where toxicity, stagnation, and deficiency are addressed rather than suppressed.
Amandha is also recognised for her uncompromising stance on germ theory, exposing its historical fraud and explaining how so-called pathogens are not external enemies but part of the body’s natural terrain response. She teaches that health is restored through cleansing, nourishment, and unblocking communication pathways, not through fear of contagion or reliance on pharmaceuticals. Her teachings bridge science, history, and natural law, showing how the medical system functions as an institution of control rather than genuine care.
Through her platform Yummy.Doctor, Amandha offers memberships that guide people step by step to become their own doctor. This includes access to an extensive private library, structured courses, and live teaching sessions. She is designing her twelve-step program to help individuals reclaim self-reliance by learning terrain-based principles, mastering case-taking and triage skills, creating a home dispensary, transitioning off pharmaceuticals, and developing preventative practices. Members gain both the knowledge and the confidence to reject unnecessary medical interventions and embrace true health sovereignty.
Beyond medicine, Amandha’s work also touches on sovereignty and law, emphasising that reclaiming health cannot be separated from reclaiming freedom. She empowers individuals to question false authorities, understand their rights, and live in alignment with natural law. This integration of health, law, and self-ownership is the cornerstone of her mission: to inspire people to free themselves from institutional control and live with vitality, clarity, and autonomy.
As a mother, Amandha embodies what she teaches. Her daughter, born at home into water with a full lotus birth, has been raised without interventions, pharmaceuticals, or vaccines. She has never seen a medical doctor, is cared for through natural means, and is homeschooled with a terrain-based, emotionally attuned approach. Their lived experience demonstrates that natural health and sovereignty are not abstract ideals, but practical, achievable realities.
Dr. Amandha Dawn Vollmer continues to educate, write, and create in service of her mission: helping people doctor themselves, dissolve fear-based myths, and remember the wisdom of nature as the true foundation of health.
Her websites:
This information is for educational and informational purposes only and is not intended as medical advice. Always consult a qualified health professional before making any changes to your healthcare regimen.
References
American Association of Medical Colleges. “Prenatal Screenings Can Lead to False Positives, Heightened Anxiety.” AAMC News, 7 Feb. 2022, https://www.aamc.org/news/prenatal-screenings-can-lead-false-positives-heightened-anxiety.
“Baby Misdiagnosed with Trisomy 18.” Motherly, 7 Apr. 2022, https://www.mother.ly/baby/baby-health/baby-misdiagnosed-trisomy-18.
“Bridget and Nora’s Story.” Trisomy 18 Foundation, https://trisomy18.org/story/bridget-noras-story.
Capes-Davis, Amanda, et al. “Check Your Cultures! A List of Cross-Contaminated or Misidentified Cell Lines.” International Journal of Cancer, vol. 127, no. 1, 2010, pp. 1–8. https://onlinelibrary.wiley.com/doi/10.1002/ijc.25242.
“Causes of False Positive and False Negative Results of the NIPT Test.” Vinmec International Hospital, 30 June 2022, https://www.vinmec.com/eng/blog/causes-of-false-positive-and-false-negative-results-of-the-nipt-test-en.
Compatible With Love Foundation. “Stories.” Compatible With Love, https://www.compatiblewithlove.org/stories.
Freedman, Leonard P., et al. “The Misidentified Cell Line Crisis: How Misidentified and Contaminated Cell Lines Threaten the Reproducibility of Biomedical Research.” PLOS ONE, vol. 12, no. 11, 2017, e0186281. https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0186281.
“Genetic Non-Invasive Prenatal Screening Tests May Have False Results: FDA Safety Communication.” U.S. Food and Drug Administration, 19 Apr. 2022, https://www.fda.gov/medical-devices/safety-communications/genetic-non-invasive-prenatal-screening-tests-may-have-false-results-fda-safety-communication.
Liehr, Thomas. “False-Positives and False-Negatives in Non-Invasive Prenatal Testing (NIPT): What Can We Learn from a Meta-Analyses on >750,000 Tests?” Molecular Cytogenetics, vol. 15, article 36, 2022. https://molecularcytogenetics.biomedcentral.com/articles/10.1186/s13039-022-00621-1.
“Maternal Cell Contamination (MCC), Prenatal.” Mayo Clinic Laboratories Pediatric Test Catalog, https://pediatric.testcatalog.org/show/MATCC.
“Maternal Cell Contamination (MCC) Testing.” UW Laboratory Test Guide, https://testguide.labmed.uw.edu/public/view/MCC.
“Miracle Baby Diagnosed with Trisomy 18.” FaithPot, 2 Nov. 2020, https://www.faithpot.com/trisomy-18-miracle-story.
“NIPT False Positive: What You Need to Know.” MyNucleus, 24 Mar. 2023, https://mynucleus.com/blog/nipt-false-positive.
“NIPT: A Crash Course in Non-Invasive Prenatal Testing.” Parents, 10 Jan. 2023, https://www.parents.com/pregnancy/stages/1st-trimester-tests/nipt-a-crash-course-in-non-invasive-prenatal-testing.
“Noninvasive Prenatal Tests Often Result in False Positives—Here’s What That Means.” Parents, 20 Apr. 2022, https://www.parents.com/news/noninvasive-prenatal-tests-often-result-in-false-positives-heres-what-that-means.
Pratt, Victoria M., et al. “Maternal Cell Contamination Studies in Prenatal Diagnosis: Best Practice Guidelines.” Association for Clinical Genomic Science, 2008, https://www.acgs.uk.com/media/10786/mcc_08.pdf.
Sui, Lei, et al. “A Review of the False-Positive Rate of Noninvasive Prenatal Testing (NIPT): Analysis of 37,858 Cases.” Molecular Cytogenetics, vol. 15, article 27, 2022. https://molecularcytogenetics.biomedcentral.com/articles/10.1186/s13039-022-00612-2.
Sun, Yu, et al. “Accurate Detection of Maternal Cell Contamination in Prenatal Samples Using Whole-Exome Sequencing Data.” Clinical Chemistry, vol. 70, no. 8, 2024, pp. 1056–66. https://academic.oup.com/clinchem/article/70/8/1056/7691420.
“Wikipedia: Prenatal Testing.” Wikipedia, https://en.wikipedia.org/wiki/Prenatal_testing.
Zhang, Li, et al. “Maternal Cell Contamination in Chorionic Villus Sampling and Amniocentesis: Detection Using Quantitative Fluorescent PCR.” In Molecular Diagnosis of Genetic Diseases, Humana Press, 2018, pp. 79–88. https://link.springer.com/protocol/10.1007/978-1-4939-8889-1_8.
This is exactly the vile bullshit that killed my baby.
Such an Important Post! You're doing Good Work and I thank you.